
Lower Cranial Nerve Palsies
Poovathoor Chacko Jacob, Abdullah Al-Asmi, Arunodaya Gujjar,
Ali Al-Mamari, Abdullah Balkhair, Ranjan William
doi:10.5001/omj.2010.68
From the Department of Internal Medicine, Sultan Qaboos University Hospital,
Al Khod, Muscat, Sultanate of Oman.
Received: 21 Jan 2010
Accepted: 28 Feb 2010
Address correspondence and reprint request to: Dr. Poovathoor Chacko Jacob,
Department of Internal Medicine, Sultan Qaboos University Hospital,
Al Khod, Muscat, Sultanate of Oman.
E-mail: jacobpc@omantel.net.om
A 70 year old diabetic male presented with a three weeks history of left temporal pain radiating to the left eye and left side of the neck without any symptoms relating to the ear or nose. Two days later, the patient developed difficulty in swallowing and speaking with nasal regurgitation of fluids. Clinical examination revealed bilateral palatal weakness (more marked on the left side), bilateral weakness of sternocleidomastoids and bilateral weakness of tongue muscles (more marked on the right side). The gag reflex was diminished. There were no pyramidal or cerebellar signs and there was no neck stiffness.
MRI of the brain showed bilateral otitis media with involvement of the petrous temporal bone. In addition, the patient had osteomyelitis of the clivus with increased uptake upon gallium scanning. He was treated with intravenous ceftriaxone 4 grams daily for three weeks, moxifloxacin 400 mgm daily and voriconazole 400 mgm daily for three months. The symptoms improved, but the patient was left with tongue weakness, more marked on the right side.
QUESTIONS
- What neurological deficit does the patient have?
- What are the likely causes?
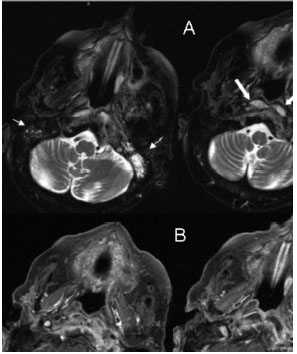
Figure 1: Panel A - T2 weighted images showing mastoiditis (thin arrows)
and preclival abscess (thick arrows)
Panel B - T1 weighted images showing hypointense bone marrow of the clivus and dural thickening
ANSWERS
- The
patient has asymmetric lower cranial nerve palsiest:normal;">The differential diagnosis of unilateral headaches includes three categories of diseases-primary headaches, intracranial and extracranial diseases. This elderly diabetic patient had no signs or symptoms of ear infection, but developed a rapid skull base osteomyelitis secondary to ear infection without any history of ear discharge. This case suggests that new onset unilateral headaches in diabetic patients should be investigated on an urgent basis with CT scan of the brain and skull base.
Seventh and eight cranial nerves are the most frequent cranial nerves involved in middle ear infections. If the infection spreads medially, the fifth and sixth cranial nerves are also invoved. Inferior extension causes a tenth cranial involvement. Acute bilateral twelfth cranial nerve, as seen in this patient is not commonly observed. Reported cases include trauma and skull base metastasis.1
Pseudomonas and aspergillus species are the most common micro-organisms seen in this condition. MRI of the skull base is the keystone to diagnosis and shows hypointensity of the bone marrow.2 Skull base osteomyelitis can be a consequence of otitis externa, media or sphenoid paranasal sinus infection
ACKNOWLEDGEMENTS
The authors reported no conflict of interest and no funding was received on this work.
-
Rotta F. Skull base metastasis causing acute bilateral hypoglossal palsy. Journal of the neurological science 1997 May; 148(1):127-129.
-
Chang PC, Fischbein NJ, Holliday RA. Central skull base osteomyelitis in patients without otitis externa: Imaging characteristics. American journal of neuroradiology 2003; 24:1310-1316.
How to cite this article
Jacob PC, Al-Asmi A, Gujjar A, Al-Mamari A, Balkhair A, William R. Lower Carnial Nerve Palsies. OMJ 2010 July; 25(3):240-241.
How to cite this URL
Jacob PC, Al-Asmi A, Gujjar A, Al-Mamari A, Balkhair A, William R. Lower Carnial Nerve Palsies. OMJ [Online] 2010 July; 25(3):240-241. Available at http://www.omjournal.org/ClinicalQuiz/201007/FT_Q_Lower%20CranialNervePalsies.html